
What is Pinched Nerve in Elbow (Cubital tunnel syndrome / ulnar neuritis)?
Cubital tunnel syndrome is entrapment of the ulnar nerve generally at the elbow. It is the second commonest cause of nerve entrapment in the body (the commonest cause is carpal tunnel syndrome with entrapment of the average nerve). The common symptoms are of numbness and tingling in the ring and little fingers and on the little finger side of the palm. It may be connected with weakening of the muscles, and in some cases losing (thinning) of the small muscles in the hand and in time contractures of the ring and little fingers might develop.
Usually the beginning is gradual, starting with numbness and tingling, particularly at night, and it might then end up being constant. Periodically the beginning may be very sudden frequently for no obvious reason. Some patients present just with weakness in the hand and others just with numbness however commonly there is a combination, especially as the condition progresses.
Why Does Pinched Nerve in Elbow Happen?
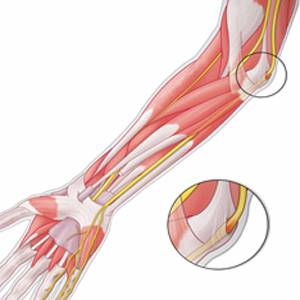
In cubital tunnel syndrome the ulnar nerve which runs behind the inner side of the elbow through a short (c. 3cm) norrow tunnel. The base and sides are made of bone from the inner of the elbow and finished by a roof comprised of a fibrous ligament. Typically the pressure in the canal is extremely low. It enhances as the elbow is bent up. Even then the pressure is not usually adequate to problem the nerve. With aging and related to different conditions such as elbow fractures (breaks) and arthritis the background pressure in the elbow increases. Any more boosts due to the posture of the elbow then results in a high adequate pressure that the blood supply to the nerve is jeopardized and it complains with symptoms of pain/numbness and tingling. In many cases the cause is unclear however it may be associated with a history of previous injury or localised underlying arthritis. Some people have a tendency to multiple entrapments and may have entrapment in the opposite ulnar nerve although this is less typical than in pinched nerve in elbow.
Pinched nerve in elbow fingers numb
In most individuals the symptoms progress progressively although on some events this can be sudden. In some individuals particularly with mild intermittent symptoms spontaneous recovery may take place. In the majority of people the numbness/tingling gradually increase leading to continuous numbness. The weakness progresses to wasting and profound weakness. These decrease hand function significantly. They generally progress together although usually the numbness or weakness will preodominate. Often just one of the numbness/weakness will exist. Therefore the symptoms of numbness, weak point and often pain will increase and become more intrusive. Many individuals are especially troubled by night waking often in the early hours of the morning.
Diagnosis for Pinched Nerve in Elbow
The Hand expert who sees the patient will ask questions about their symptoms, when they began, how they advanced, what treatment (if any) they have had and other concerns relevant to the issues. They will then examine the patient looking at the patient’s elbows, wrists and hands and normally likewise their neck as this can give numbness and tingling in the hands. Special medical tests such as tapping over the nerve and holding the elbow bent are performed to try to reproduce the symptoms to assist validate the diagnosis.
What test(s) might be carried out?
Tests (also known clinically as Investigations) consist of X-rays, scans, blood tests and especially in the hand electrical tests (called EMGs or Neurophysiology). These may be used to help make or validate a medical diagnosis after a patient has explained their symptoms and been examined.
In ulnar neuritis the medical diagnosis is normally apparent after paying attention to and analyzing a patient. Often the cosmetic surgeon will arrange an X-ray of the elbow however that is not regular. The commonest test is an electrical test. It is almost always requested if surgery is planned. This is carried out at a later date by a specialist (Neurophysiologist). Moderate electrical shocks are sent up and down the arm and the strength and speed of their conduction is determined. This gives a measure of nerve function. Like all tests it is not totally trusted so it can be normal although the patient has ulnar neuritis and it can be unusual when the patient does not have ulnar neuritis. Your Hand professional will analyze the results in the light of the previous description of symptoms and examination and advise you appropriately.
The other typical possible causes of the symptoms are nerve entrapment in the neck and pinched nerve in elbow.
Treatment for Pinched Nerve in Elbow
What are the non-operative treatments?
Treatment ought to begin with non-operative options. These consist of activity modification (which usually does not offer much advantage or has already been tried by the patient) and an elbow night extension splint. The splint is primarily worn during the night to avoid waking. It limits the elbow from bending up far therefore helps protect the nerve from being squeezed in the evening. Avoidance of prolonged flexing of the elbow is also handy such as preventing utilizing the arm to hold the phone for long term durations.
Pinched nerve in elbow & surgery
The operation is called an ulnar nerve decompression. We often perform the operation under local anaesthetic in a strategy we developed and have actually reported in the clinical literature. A band, like a blood pressure cuff, is put around the top of the arm. It is inflated (tightened) during the operation to decrease bleeding, that makes the operation much easier and much safer. It can be a little unpleasant, but is often well tolerated for the 15-20 mins or two that it is inflated (this happens right before the specialists starts the operation). Before that the arm is painted with an antibacterial with a pink dye in it. This is used to assist reduce the risk of infection.
A cut of 1-1.5 inches (3-4cm) is required, just behind the bony prominence on the inner side of the elbow. If, at the end of the release, the nerve is tending to ride forwards a lot, this, too, can cause more issues and part of the bony prominence on the inner side of the elbow (medial epicondyle) will be gotten rid of. This enables the nerve to sit in a more comfy position, reducing the chances of frequent compression or a bad result. If, nevertheless, the nerve sits nicely, then this additional procedure would not be undertaken as it enhances the pain in the initial post-operative period. Hardly ever the nerve will need to be officially gotten rid of in front of the medial epicondyle (prominent bone). If this is needed it will have been recognized pre-operatively and the operation will need to be performed under a basic anaesthetic, as a significantly longer incision will be required. At the end of the operation the wound is sewn usually with absorbable stitches. A helpful dressing is applied and the patient’s arm elevated.
The total time in health center is usually 2-3 hours.
What happens in the next few weeks?
The care of the hand in the post-operative period is essential in assisting to guarantee a good outcome. At first the goals are comfort and elevation. These are fulfilled by keeping the hand up (raised) particularly in the first few days and by utilize of a long acting regional anaesthetic (Bupivicaine). The regional anaesthetic lasts at least 12 hours and often 48 hours. Patients must begin taking painkillers prior to the pain begins i.e. on return home and for a minimum of 24 hours from there. This way most of our patients report little or any pain.
The bandage can be eliminated after 2-7 days, leaving a sticky dressing beneath. The patient or GP practice nurse can do this. If well healed at that stage then the injury can be left open (exposed). If in doubt it can be covered with a light dressing for a couple of more days. The patient is evaluated in center in between 2-4 weeks following the operation. Generally dissolvable stitches are used so they must not need to be eliminated.
The hand can be used for typical activity after the first couple of days. The majority of patients can drive after a week or two. Many patients return to operate in 2-3 weeks, however this varies with occupation; heavy manual labor normally takes about 6 weeks. The injury must be rubbed by the patient 3 times a day with a boring soft cream for 3 months as soon as the injury is well recovered (normally after 2 weeks). This lowers the scar sensitivity which can be a nuisance. If this is marked a Physio may be arranged to assist decrease the scar tenderness however this is seldom required. Patients ought to avoid pressing heavily on the scar for 3 months following the operation as this will be quite painful.
What are the outcomes of the operation?
The goal of the operation is primarily to prevent the condition deteriorating even more with recovery a secondary goal. By these criteria at least 85 % of patients in research studies say they have a good or excellent outcome following this operation, with relief of the pain and no progression of their symptoms. In the majority of patients there is at least partial recovery of their symptoms. Recovery of full nerve function is unreliable. This may be due to the fact that the nerve is trapped even more far from where the hand requires the supply or because patients generally come for surgery with more established continuous symptoms. It might take 2 years for the improvement in feeling, muscle bulk and stamina to optimise.
Risk factors
All interventions in medication have threats. In basic the bigger the operation the higher the risks. For ulnar neuritis the risks consist of:
- The scar may be tender, in about 20 % of patients. This normally improves with scar massage, over 3 months.
- Aching in the elbow generally settles within 1-2 months. Grip stamina can also take a couple of months to go back to normal.
- Tightness might occur in particular in the elbow. This is generally short-term and only occasionally requires physiotherapy.
- Numbness can occur around the scar but this hardly ever causes any practical problems.
- Wound infections happen in about 1 % of cases. These typically quickly resolve with antibiotics.
- Recurrence – Recurrent symptoms are recorded. They may happen due to additional deterioration in the elbow if there is a hidden problem or for factors that are not completely clear. The risk of reoccurrence is of the order of 2-5 % in the long term. Frequently this will settle or at least enhance with redo surgery.
- Chronic Regional Pain Syndrome “CRPS”. This is an uncommon but serious problem, with no recognized cause or tested treatment. The nerves in the hand “over-react”, triggering swelling, pain, discolouration and stiffness, which enhance extremely gradually.
- Any operation can have unforeseen effects and leave a patient even worse than before surgery.








Those who suffer from CTS are priced between those people who are mildly inconvenienced and must wear a splint at night to alleviate stress on the median nerve to people who are severely debilitated and shed usage of their fingers. Problems associated with CTS can invade someone’s life making even simple tasks such as for example answering the telephone, reading a book or opening a door very difficult. In serious cases, surgery to discharge the median nerve is oftentimes suggested by an orthopedist. The carpal tunnel ligament is cut, relieving the pressure inside the carpal tunnel. Rates of success are quite high with all the surgical procedure.
To understand more just how I handle it you certainly can do a search that is google carpal tunnel exercises Aaron wix Jones to get the site which we used