After gallbladder removal, some abdominal pain may appear years later. We will tell you about how these pains are related to a person’s missing gallbladder.
What Is Pain Years After Gallbladder Removal Mean?
Many people who have had their gallbladders removed through surgery may still suffer from symptoms, including pain, even after several years. This prolonged pain can have multiple potential causes, which will be explored further in the following explanations.
- Post-Cholecystectomy Syndrome (PCS)
Post-cholecystectomy syndrome, also known as PCS, is a collection of symptoms that occur after the gallbladder has been surgically removed. Abdominal pain, bloating, diarrhea, and indigestion, along with other indications, are some of the symptoms that one may experience. Statistics suggest that around 40% of individuals who undergo gallbladder removal may encounter PCS, with the possibility of it appearing months or even years after the operation.
- Sphincter of Oddi Dysfunction
The Sphincter of Oddi is responsible for regulating the passage of bile and pancreatic juice into the small intestine. Occasionally, this particular muscle may experience heightened sensitivity or involuntary contractions, resulting in discomfort in the upper right section of the abdomen. This medical issue is called Sphincter of Oddi Dysfunction and may develop following the removal of the gallbladder.
Health Support: This Vitamin K2 + D3 Complex is essential for bone density, cardiovascular health, and immune function. It’s a highly-rated formula for those looking to maintain optimal nutrient levels. You can find it on Amazon.
- Adhesions
Scar tissue bands known as adhesions can develop within the abdomen following surgery, resulting in discomfort. These adhesions may cause pain by exerting pressure on organs or trapping nerves. In addition, they can form after the removal of the gallbladder and continue to cause pain for several years post-surgery.
- Other Conditions
There are several other conditions that can cause abdominal pain and discomfort, including irritable bowel syndrome (IBS), ulcers, and gastroesophageal reflux disease (GERD). These conditions can develop at any time, including years after gallbladder removal surgery.
How to Recognize the Pain Years After Gallbladder Removal
Although the majority of individuals find relief from their symptoms following gallbladder removal surgery, some may still encounter pain and discomfort that could be associated with the procedure.
How can you determine if the pain or discomfort you are feeling is connected to your gallbladder removal surgery, particularly if it occurred multiple years ago? Here are a few factors to consider.
Health Support: This high-absorption Magnesium Glycinate (200 mg) is gentle on the stomach and supports muscle relaxation, better sleep, and metabolic health. You can find this trusted formula on Amazon.
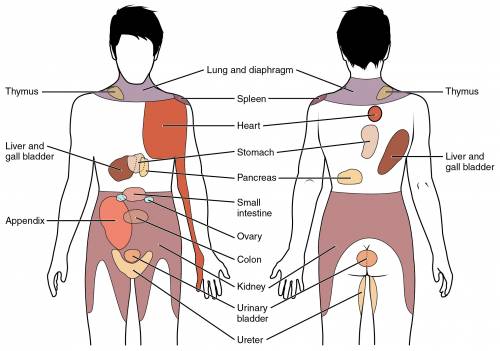
- Location of the pain: If you feel any pain or uneasiness on the upper right part of your abdomen, specifically where your gallbladder was removed, it might indicate that the pain is linked to your surgery. However, it is worth remembering that this particular area of the abdomen can also be associated with other problems like liver issues or kidney stones. That is why it is crucial to consult your doctor if you are experiencing any form of abdominal pain.
- Timing of the pain: If you experience pain or discomfort following a meal, it could indicate that it is connected to your gallbladder. This is because the gallbladder’s role is to store and release bile, which aids in digestion. Without a gallbladder, bile may go directly into the small intestine, leading to discomfort or pain.
- Other symptoms: Besides experiencing pain or discomfort in the upper right area of the stomach, there are other indications that could potentially be connected to the removal of the gallbladder, such as diarrhea, indigestion, and bloating.
If you’re experiencing any of these symptoms and you’re concerned that they may be related to your gallbladder removal surgery, it’s important to speak with your doctor. They can perform tests such as an abdominal ultrasound, endoscopy, or CT scan to determine the cause of your symptoms.
Sometimes, the pain or uneasiness you experience might not be connected to the removal of your gallbladder, but rather to a separate issue like a hernia or strained muscles. Nevertheless, if the pain is a result of your surgery, there are methods of treatment accessible. Your physician might suggest medications or alterations to your diet to assist in controlling your symptoms.
Treatment Options
- Medications:
To alleviate pain and discomfort, your physician might recommend the use of medications like antispasmodics, painkillers, or bile acid binders.
- Dietary changes:
Limiting your fat intake, avoiding caffeine and quitting alcohol, and eating smaller meals can help alleviate symptoms associated with SOD and IBS.
- Endoscopic Retrograde Cholangiopancreatography (ERCP):
ERCP is a medical procedure that involves inserting a scope into the bile duct to identify and treat any blockages that may be causing pain and discomfort.
Health Support: The WHOOP 5.0 Activity Tracker offers a comprehensive, 24/7 analysis of your body’s recovery, sleep patterns, daily strain, and key health biometrics. It’s an invaluable tool for anyone looking to optimize their energy, manage stress, and understand what their body truly needs. You can find it on Amazon.
- Surgery:
In some cases, surgery may be necessary to treat pain caused by adhesions or other complications.
Prevention
While there is no sure way to prevent pain years after gallbladder removal, implementing healthy lifestyle changes can reduce your risk of developing complications. These may include:
- Eating a healthy diet
- Exercising regularly
- Limiting or avoiding the consumption of caffeine and quit alcohol
- Consulting with your healthcare provider before taking any medications.