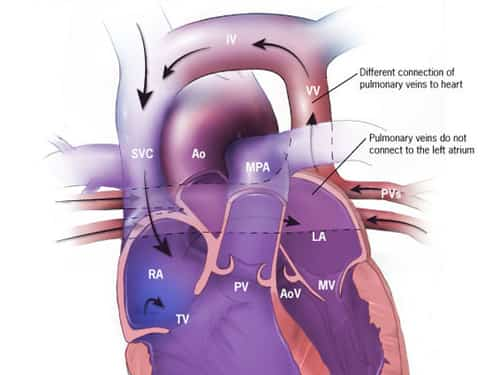
In TAPVD, rather than carrying oxygen-rich blood from the lungs to the left atrium of the heart, the pulmonary veins are linked to the right atrium or veins that lead to the right atrium. This leads to a mixing of oxygen-rich and oxygen-poor blood, which results in a less effective distribution of oxygen throughout the body.
Anatomy of TAPVD
The anomaly typically arises from an improper development of the pulmonary veins during fetal growth. Here’s a breakdown of what happens in this condition:
- Pulmonary Veins: These vessels are responsible for transporting oxygenated blood from the lungs to the heart. However, in TAPVD, they do not connect to the left atrium.
- Abnormal Drainage Site: The pulmonary veins instead connect to either the right atrium directly, the superior vena cava, the inferior vena cava, or the coronary sinus.
- Atrial Septal Defect (ASD) or Patent Foramen Ovale (PFO): Typically, in cases of Total Anomalous Pulmonary Venous Drainage in infants, there is often a presence of either an Atrial Septal Defect or a Patent Foramen Ovale, which enables a partial mixing of oxygen-rich and oxygen-poor blood, thereby ensuring some level of oxygen supply to the body.
Causes
The cause of TAPVD is not fully understood, but several factors may play a role:
- Genetic Factors:
- Mutations in specific genes such as GATA4 and NKX2-5 may contribute to the development of TAPVD.
- Family history of congenital heart defects can increase the risk of an offspring developing TAPVD.
- Chromosomal Abnormalities:
- TAPVD is sometimes associated with chromosomal anomalies, such as Down syndrome (Trisomy 21).
- Environmental Factors during Pregnancy:
- Maternal exposure to certain substances or conditions during pregnancy, such as certain medications, illegal drugs, alcohol, or viral infections, may increase the risk of a child being born with TAPVD.
- Maternal Health Conditions:
- Diabetes mellitus or lupus in the mother can be linked to a higher incidence of congenital heart defects like TAPVD.
- Abnormal Fetal Development:
- TAPVD occurs during the first eight weeks of fetal development when the heart is forming. An interruption or anomaly in the development of the pulmonary veins can lead to TAPVD.
- Teratogen Exposure:
- Exposure to teratogens—agents that cause malformations of an embryo—such as certain prescription drugs, over-the-counter medications, or environmental toxins, might contribute to the formation of TAPVD.
- Nutritional Deficiencies:
- Some studies suggest that a lack of certain nutrients during pregnancy, including folic acid, might be associated with an increased risk of congenital heart defects, including TAPVD.
- Unknown Factors:
- In many cases, the exact cause of TAPVD remains unknown. This idiopathic nature suggests there may be other unknown factors or a combination of factors at play.
Types of TAPVD
TAPVD is categorized into four types according to the site of drainage:
Health Support: This Vitamin K2 + D3 Complex is essential for bone density, cardiovascular health, and immune function. It’s a highly-rated formula for those looking to maintain optimal nutrient levels. You can find it on Amazon.
- Supracardiac: The pulmonary veins carry blood to the right atrium through the superior vena cava.
- Cardiac: The pulmonary veins empty into the right atrium either directly or through the coronary sinus.
- Infracardiac: The pulmonary veins empty into the right atrium by way of veins that join with the inferior vena cava.
- Mixed: The pulmonary veins can either empty into both the superior and inferior vena cava, or into various other locations that are not typical.
Common Symptoms
Infants with TAPVD may exhibit several symptoms shortly after birth, including:
- Cyanosis (bluish skin due to lack of oxygen)
- Difficulty breathing
- Feeding difficulties
- Poor weight gain
- Fatigue
- Rapid breathing or shortness of breath
Diagnosis and Treatment
TAPVD is typically diagnosed through a combination of physical examination, imaging studies, and heart tests including:
- Chest X-ray: Can show the size and shape of the heart and the lung fields.
- Echocardiogram: A key tool that uses sound waves to create images of the heart, revealing the abnormal pulmonary veins.
- Cardiac MRI or CT Scan: Offers detailed images of the heart and blood vessels.
- Cardiac Catheterization: May be used to measure the pressures inside the heart chambers and blood vessels.
The definitive treatment for TAPVD is surgical correction, ideally performed shortly after diagnosis. The surgery involves:
- Reattachment of the Pulmonary Veins: The pulmonary veins are detached from their abnormal connection and reattached to the left atrium.
- Closure of ASD or PFO: If present, the ASD or PFO is closed to normalize the flow of blood through the heart.
Prognosis
With early detection and surgical intervention, many children with TAPVD can lead normal, active lives. However, long-term outcomes depend on the complexity of the condition, the presence of associated defects, and the timing of the surgery.
Health Support: This high-absorption Magnesium Glycinate (200 mg) is gentle on the stomach and supports muscle relaxation, better sleep, and metabolic health. You can find this trusted formula on Amazon.
Monitoring and follow-up care are crucial to manage any complications and to ensure that the child’s heart is functioning properly as they grow. Advances in surgical techniques continue to improve the prognosis for individuals with Total Anomalous Pulmonary Venous Drainage.